What is FGM/C?
Female genital mutilation/cutting (FGM/C) is a harmful practice involving the full or partial removal, or injury to a girl’s external genitals. On average, girls are subjected to FGM/C before the age of five, although this varies between different communities and can happen at any time from a girl’s birth to her adolescence.
FGM/C is not an obligation of any religion and has no known health benefits. Far from it, the practice can cause long-lasting physical and psychological damage for more than 230 million women and girls who are affected worldwide. In some cases, this can include death.
FGM/C is a global concern
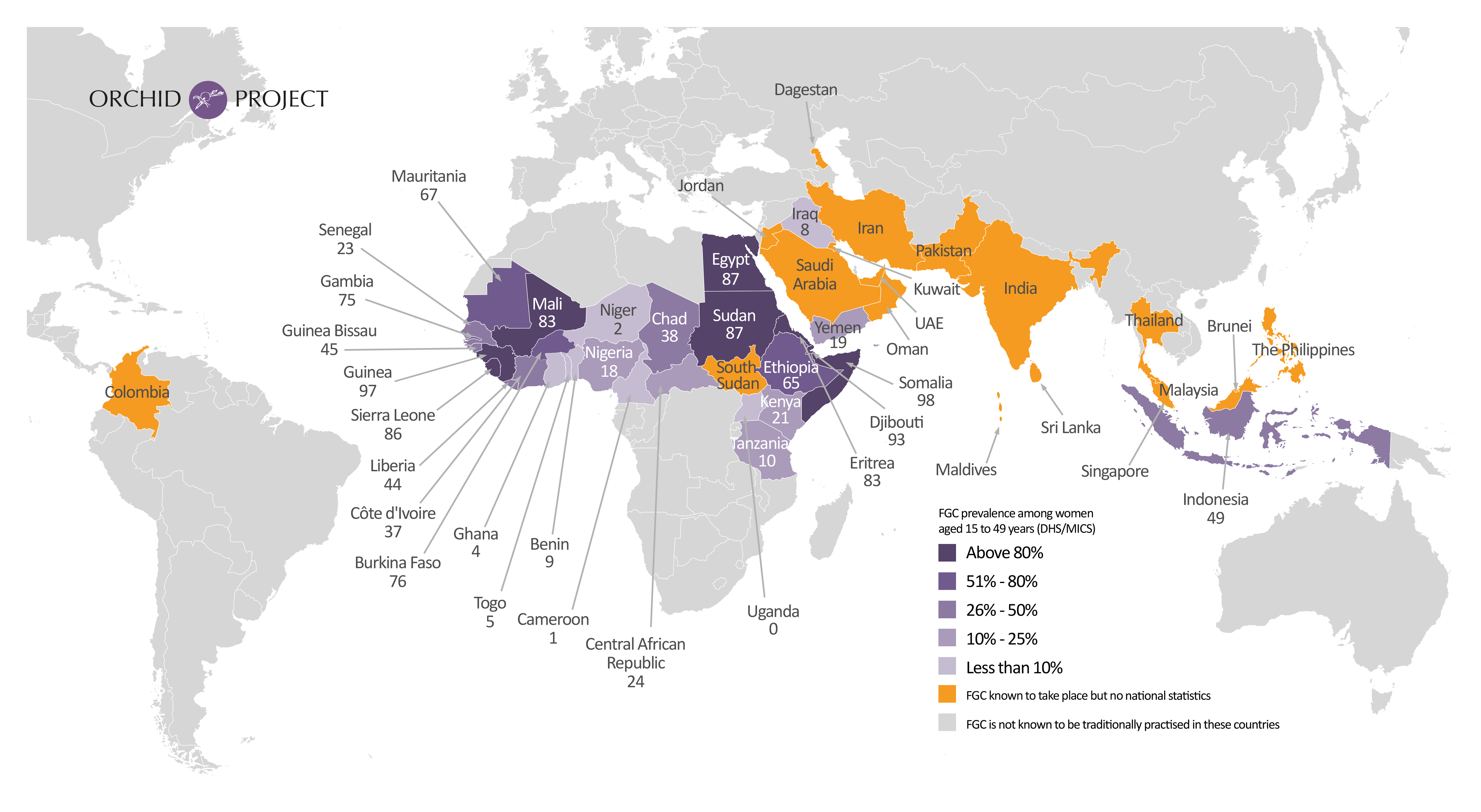
It is estimated that more than 200 million women and girls have undergone female genital cutting. This figure is based on the 32 countries that measure and report on the practice, across three continents. We know, however, that girls are affected by FGM/C in over 90 countries globally, so this figure underestimates the true scale of the practice. FGM/C takes place in Africa, the Middle East and Asia, and also within diaspora communities around the world.
Estimates suggest 4.1 million girls a year are at risk of being cut. And although global efforts to encourage communities to abandon FGM/C are making strong progress, population growth means the number of girls at risk of being cut continues to increase.
Also referred to as female genital mutilation (FGM) and female circumcision, the practice of cutting is recognised internationally as a violation of human rights, the rights of the child and women’s rights.
 +230 million
+230 million
women and girls are
impacted by FGM/C
 FGM/C occurs in over
FGM/C occurs in over
90 countries
globally
 girls are at risk
girls are at risk
each year
{kind=link}
What FGM/C entails
Female genital cutting as a term encompasses a range of harmful procedures that involve partial or total removal of a girl’s external genitals, or other injury to the female genital organs for non-medical reasons.
FGM/C can often be carried out by ‘traditional practitioners’, such as birth attendants, who have little or no access to information about human rights and no medical training or knowledge of the potentially dangerous medical and psychological impacts of FGM/C on the girls they cut. It often takes place in unsterile, domestic environments, using unsafe tools.
Increasingly in certain settings around the world, girls undergo FGM/C at the hands of trained health care providers due to the mistaken belief that the procedure is safer when medicalised.
There are 4 types of FGM/C
Type I
The clitoris or clitoral hood is partially or fully removed (clitoridectomy).
Type II
As well as the clitoris, the labia minora (inner vaginal lips) are partially or fully removed. The labia majora (outer lips) may also be cut.
Type III
The clitoris, labia minora and labia majora are cut away, and the remaining skin is sewn or sealed together leaving a tiny hole for menstrual blood and urine (infibulation).
Type IV
All other harmful procedures to the female genitals including pricking, piercing, rubbing, scraping and cauterisation.
All types of FGM/C are a violation of human, child and women’s rights, and can lead to a range of physical and psychological consequences.
*World Health Organisation definitions
An urgent human rights issue
Efforts to end FGM/C are growing globally, but population growth and the continuation of the practice around the world make it an increasingly urgent human rights issue.
 1 in 3 girls worldwide will be born in the 30 countries where FGM/C is concentrated by 2030.
1 in 3 girls worldwide will be born in the 30 countries where FGM/C is concentrated by 2030.
 22 of the 30 countries that report national data on FGM/C prevalence have the lowest socioeconomic development indicators.
22 of the 30 countries that report national data on FGM/C prevalence have the lowest socioeconomic development indicators.
 68 million girls are at risk of being cut between 2015 and 2030 unless efforts to end the are accelerated.
68 million girls are at risk of being cut between 2015 and 2030 unless efforts to end the are accelerated.